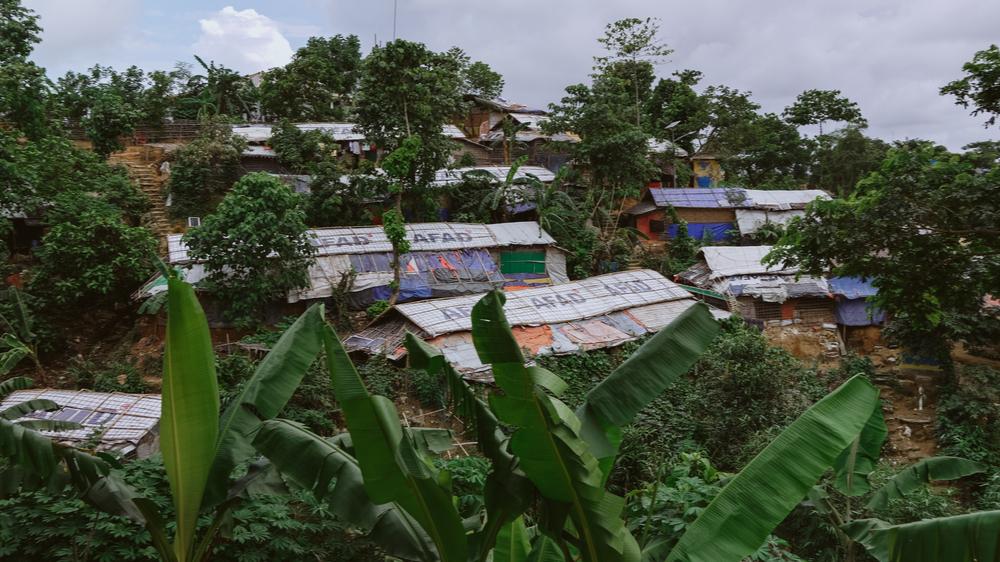
The bamboo and tarpaulin shelters were built as temporary solutions. Many Rohingya families fled Myanmar thinking they would return to their homes within a few months. ©Victor Caringal/MSF
Scabies is a parasitic infection caused by microscopic mites (Sarcoptes scabiei) that burrow under human skin and lay their eggs. The skin doesn’t take kindly to this infestation, which leads to an angry, itchy rash. While it is not fatal, it lowers the quality of life, especially to those who have no proper housing or ability to treat. The intense itching can lead to sleepless nights and, in turn, poor mental health outcomes.

A young patient from Rohingya refugee camp is visiting Doctors Without Borders’s Jamtoli facility to seek treatment of scabies. ©MSF/Malvoisin
What else could be expected to happen when containing one million refugees indefinitely in temporary camps?
The question now is less about why the world ignored the warning signs, but what it will take for the international community, donors, and the United Nations to take more responsibility for the Rohingya.
I have worked with the Rohingya community for more than six years. The Doctors Without Borders teams have provided healthcare to vulnerable Rohingya in their homeland, Myanmar since 1993 and have seen the successive failings of international responsibility.
Controlling this scabies outbreak would require a mass drug administration, plus effective vector control in the entirety of the camps. Essentially this would require every household cleaning their bedding and clothes at the exact same time. None of this is possible for the Rohingya, who have less than adequate water supply and soap allocation in the crowded camps.
The camps were only meant to be a short-term option. But after six years, temporary structures are becoming longer term liabilities, resembling slums rather than homes. Without a change in the unsustainable containment strategies of donor governments, and host government, the camp population will remain acutely vulnerable to outbreaks of infectious disease.

Inadequate access to safe water and poor sanitation conditions compound health risks in the overcrowded camps, enabling outbreaks like scabies. ©Victor Caringal/MSF
This latest scabies outbreak should be enough for international governments to work towards durable solutions with greater urgency and determination. But sadly not. It feels absurd to justify why this outbreak is an undignified public health crisis no population should have to endure.
Beyond scabies, the nutritional situation in the camps is also parlous. We are worried about the number of malnutrition cases reaching our clinics in the camps. In 2022, in just two of our facilities, we counted 3,200 cases of malnutrition among pregnant and lactating women, of which 40 per cent were anaemic, and 25-28% of babies born were of low birth weight. General acute malnutrition rates among children under five years were at 19 per cent in 2022, and 21 per cent up until mid-2023.
Combine this with World Food Programme reducing the food allowance for the Rohingya to US$8 a month , we would expect increasing level of malnutrition and anaemia, higher rates of low-birth-weight babies and in-turn higher mortality rates among women and children. There is an entire generation of Rohingya children facing the possibility of stunted growth due to lack of sustained nutrition. The same children are also denied the right to a full education. The Rohingya refugee camps in Cox’s Bazaar in Bangladesh seem to be a place where humanitarian standards don't apply, largely forgotten and neglected by the rest of the world.
An entire generation of women, children and men who are reduced to simple words like "refugees" or "stateless people". They are more than that, they are people who have endured persecution, seen their villages burned, family members killed, only to face a life behind barbed wire fences in conditions you nor I will probably ever endure. They are people surviving every day, despite these circumstances, as mothers, fathers, daughters and sons. They are people like the rest of us, as artists, teachers, carers and much more.
Precarious situations in refugee camps can often occur when there is an inability or unwillingness of international organisations to be aware of threats that arise gradually. In the case of the Rohingya in Bangladesh, in fact there are one million urgent reasons not to be complacent.







