
A Rohingya woman fills a pot with drinking water at a water point in Kutupalong-Balukhali camp in Cox’s Bazar district. Bangladesh, July 2022. © Elizabeth Costa/MSF
Background
In 2017, over 700,000 Rohingya people were uprooted by a massive campaign of targeted violence in Myanmar and crossed the border into Cox’s Bazar, Bangladesh, where they joined more than 200,000 Rohingya who had taken refuge there in previous years. The Bangladeshi authorities built shelters of bamboo and plastic to host the new arrivals over a 25 square kilometre area of hilly forest terrain, an area that has become the largest refugee camp in the world.
To provide the Rohingya with emergency access to water and sanitation, boreholes were dug, water points were established and latrines were installed.
As well as being one of the major providers of medical care in the camps, Doctors Without Borders has been one of the key parties supporting the development and maintenance of water and sanitation facilities since 2017. In 2020, we adapted our water and sanitation activities to ensure the longer-term sustainability of these services. This involved handing over most of our water and sanitation activities to local organisations, including an extensive water network using solar energy to power clean drinking water. We continue to collaborate closely with relevant water and sanitation operators in the camps to provide support in addressing critical maintenance gaps in these services.
Doctors Without Borders first conducted a community feedback study in 2018 to understand the availability and quality of water and sanitation services in the camps, and to identify gaps. In 2022, after witnessing a clear increase in patients requiring treatment for skin infections, such as scabies, and water-borne illnesses, such as acute-watery diarrhoea, Doctors Without Borders decided to replicate the 2018 study to understand how services have developed and what gaps remain.

Access to clean water and toilet facilities are one of the most critical issues for the million Rohingya refugees living in Cox’s Bazar’s mega-refugee camp and more efforts are needed to improve access to clean water and toilet facilities. Bangladesh, June 2022. © Saikat Mojumder/MSF
The study
The 2022 water and sanitation community feedback study is part of a regular monitoring and community feedback mechanism focused on access to water, hygiene and sanitation services in the Cox’s Bazar refugee camps. The 2018 study provided a baseline for analysing the water and sanitation conditions.
The purpose of both assessments was to determine the access to water and sanitation services for Rohingya refugees, and to identify gaps in service provision and health impacts associated with these gaps. They were based on the same lot quality assurance sampling (LQAS)[1] methodology, which made it possible to compare the 2018 and 2022 findings, identify areas of improvement of the situation since 2018, establish where conditions had deteriorated, show persistent gaps, and put forward recommendations.
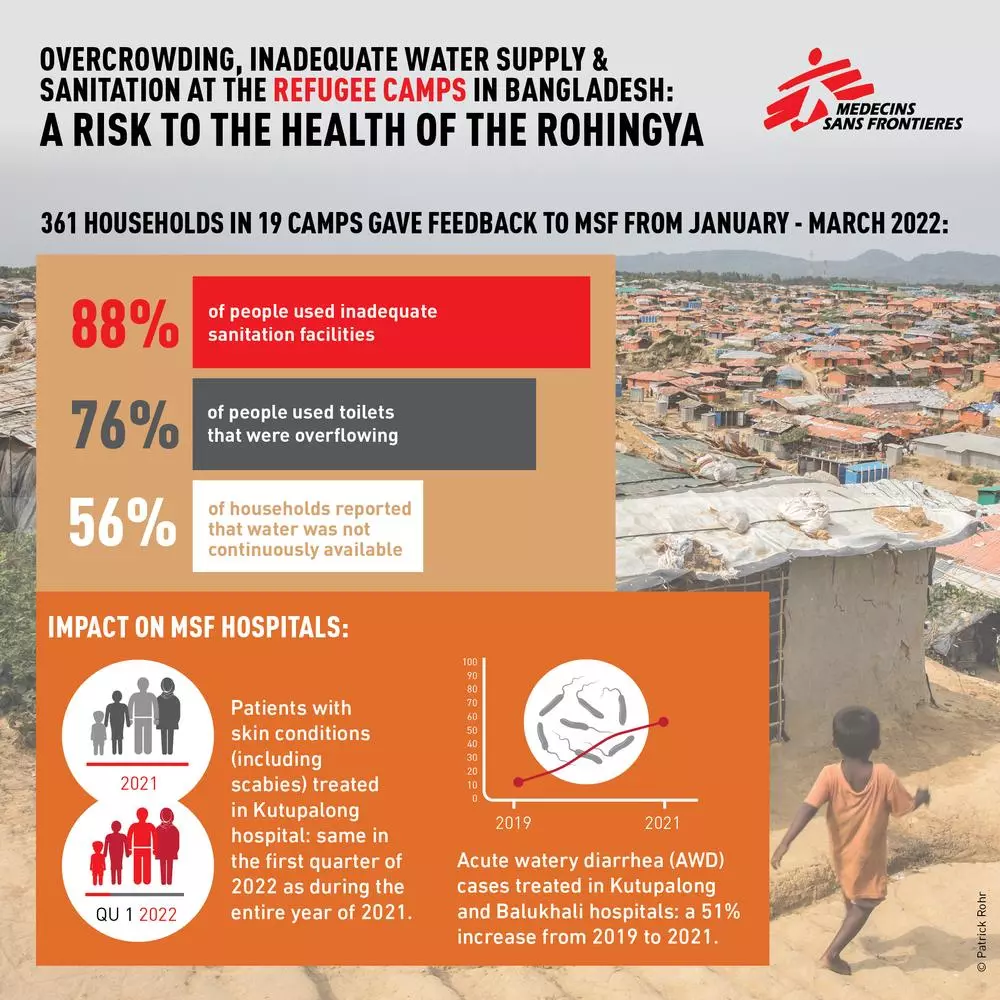
In 2018, 399 households across 21 of the camps were asked to provide feedback over a period of 35 days during October and November. In 2022, Doctors Without Borders consulted people in 361 households across 19 camps, over 18 days during January and March.
Key findings
The study showed an improvement in water quality in 2022 compared to 2018, and a functioning waste collection system. However, it also found a reduction in the number of functioning latrines and deterioration of waste collection.
Three-quarters of the households interviewed reported that latrines were overflowing. Over half said there were visible feces and that their water supply was limited. A quarter of the households also indicated a shortage of containers for waste disposal.
- A total 99% of respondents indicated that they had access to improved quality of water, compared to 53% in 2018, due to the installation of water networks and the use of chlorination. However, 56% of people indicated that water was not always available.
- While more lockable doors and covers for openings had been installed, 76% of respondents indicated that toilets were overflowing, compared to 38% in 2018. It was reported that latrines were not being de-sludged or maintained in a timely manner.
- Of respondents, 24% also reported a shortage of containers for disposal of household waste.
Health related results
The study indicated a deterioration in people’s health linked to the unsanitary situation in the camps.
- Of the households interviewed, 31% reported skin infections (an increase from only 7% in 2018).
- A total 21% of households reported diarrhoea among children under 5 years.
The accumulation of contaminated water in the camps was found to be a breeding environment for mosquitoes that spread malaria and dengue. During June and July of 2022 alone, Doctors Without Borders facilities admitted 248 patients with dengue to our facilities for treatment. In 2018, primary infections of dengue were rare in Cox‘s Bazar District.

Water and sanitation facilities built by Doctors Without Borders in Jamtoli camp for Rohingya refugees, Cox’s Bazar. Bangladesh, 2019. © Anthony Kwan/MSF
Conclusions and recommendations
- The feedback study findings indicate that while the quality of water has improved, there is insufficient access to water.
- The overall sanitation situation in the camps has deteriorated over the last four years, posing health risks to refugees and impacting their ability to live with dignity.
- Inadequate disposal of waste from people’s shelters risks attracting rats and turns the shelters into potential breeding sites for mosquitoes, which transmit diseases such as dengue.
Urgent action is needed to address these new and re-emerging risks linked to inadequate water, hygiene and sanitation services.
Doctors Without Borders recommends that:
- Humanitarian organisations providing water and sanitation services routinely and systematically maintain sanitation facilities to ensure their usability. In addition to improving the quality and availability of water, organisations must also guarantee their functionality. Clinical treatment is not enough to address vector-borne diseases such as dengue: fumigation and larval source management are needed.
- Donors contribute to the provision of effective and adequate water and sanitation services for the Rohingya community by including operational standards and facility maintenance in funding requirements linked to accountability.
- Camp management authorities engage in facilitating more robust coordination and effective implementation of the water and sanitation response, and remove restrictions on the provision of water in the camps to ensure that all communities have equal access to sufficient water.
Doctors Without Borders is working with water, sanitation and hygiene providers in Cox’s Bazar, and relevant donors, to improve the quality and availability of water, sanitation and hygiene services. Doctors Without Borders believes that all stakeholders must work to develop collaborative solutions to this humanitarian situation.
We have shared the key findings and recommendations with agencies and organisations leading the water and sanitation response, as well as partners delivering services. Additionally, Doctors Without Borders contacted donors and camp management officials to discuss the results of the report and our suggestions for how they can facilitate implementation and coordination.
At this pivotal point where parties to the response in Cox’s Bazar are developing their strategies for the coming period, it is essential for Doctors Without Borders and other responders urgently reaffirm their commitment to improving water, sanitation and hygiene services so that the health of the Rohingya community in Bangladesh does not deteriorate further.







